


Suicide in the Australian Defense Force, 1997-2021
Graph of the Week

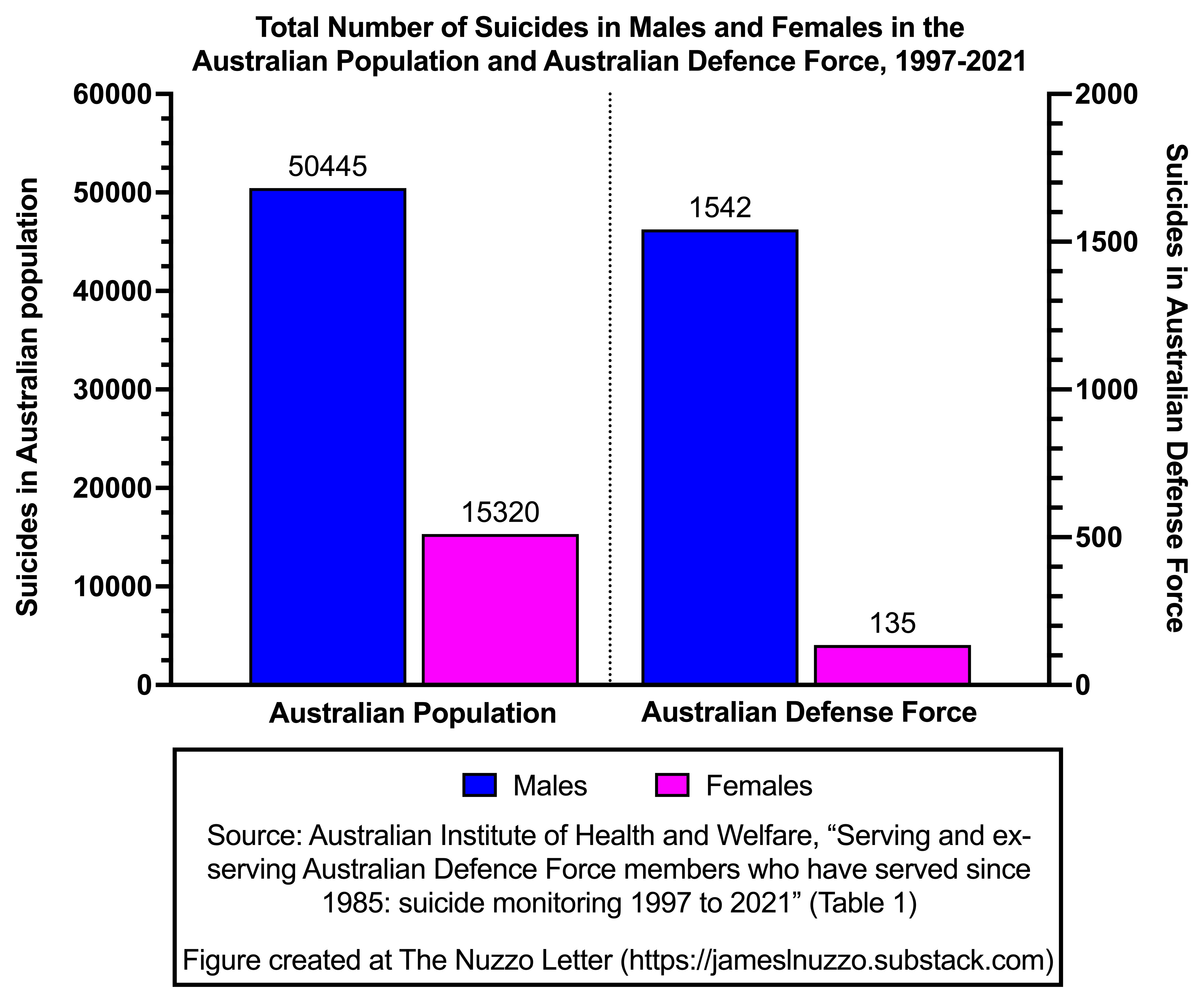
This week’s graph, based on a report by the Australian Institute of Health and Welfare, shows the number of male and female deaths by suicide in the general Australian population and in the Australian Defence Force (ADF) between 1997 and 2021. The data from the ADF include serving, reserve, and ex-serving members.
Key Points
Between 1997 and 2021, 65,675 individuals died by suicide in Australia. Approximately 77% of these individuals were male and 23% were female.
Between 1997 and 2021, 1,677 members of the ADF died by suicide, accounting for 2.6% or about two out of every 100 suicides in Australia. Approximately 92% of suicides among ADF members were males.
Source: Australian Institute of Health and Welfare. (2023). Serving and ex-serving Australian Defence Force members who have served since 1985: suicide monitoring 1997 to 2021.
Bonus Commentary
Males are three out every four suicides in the general Australian population and about nine out of every 10 suicides in the ADF. Higher suicide rates in males than females are observed in all countries. Higher rates of suicide among military veterans than the general population are observed in Australia and the United States.
A literature review published by the Centre for Social and Early Emotional Development at Deakin University identified the following barriers to men’s help seeking for mental health issues:
Individual barriers
Masculine norms (e.g., perceptions of being weak, losing control, or not being self-reliant if one consults with a mental health professional)
Stigma (e.g., belief that seeking help could lead to social exclusions, judgments, or bullying)
Challenges with articulating emotions
Low mental health literacy (e.g., lack of awareness of one’s mental health state, lack of understanding of the importance of mental health, not understanding what is involved with consultations)
Sense of fear or uncertainty (e.g., fear of hospitals, negative beliefs about treatments, lack of desire to complete questionnaires)
Health system barriers
Availability of services (e.g., navigating the health system, unsure where to find information or services)
Lack of male-specific services
Issues or limited previous experience with health professionals
Cost of health services or lack of insurance coverage
Health services offered only during traditional work hours
Other barriers
Lack of time to see a health professional
Travel distances involved for men living in rural or remote areas
Language barriers
Related Content at The Nuzzo Letter



SUPPORT THE NUZZO LETTER
If you appreciated this content, please consider supporting The Nuzzo Letter with a one-time or recurring donation. Your support is greatly appreciated. It helps me to continue to work on independent research projects and fight for my evidence-based discourse. To donate, click the DonorBox logo. In two simple steps, you can donate using ApplePay, PayPal, or another service. Thank you!

Sadly, suicide is yet another stark example of men’s issues getting hijacked.
The problem starts by conflating suicide and mental health. This is smoke and mirrors. There is clear evidence that most male suicide isn’t associated with mental health problems, it’s caused by men’s lives being literally unendurable – often due to the viciousness of the Family Law system. But none of this gets talked about – least of all by the feminist bureaucrats in National Suicide Prevention Office & National Mental Health Commission.
The result is that money intended to help men ends up diverted to women e.g. into anorexia.
The AIHW study found that ADF ex-serving men who separate for involuntary medical reasons are around three times as likely to die by suicide as men who separate voluntarily, otherwise ex-serving men have only a small elevated risk of dying by suicide compared to Australian men. Other groups in society have higher rates of suicide or attempted suicide than ex-serving men and women but receive none of the concern or assistance lavished on them. For example, people with autism attempt suicide at approximately nine times the rate of neurotypical people. People who are adopted attempt suicide at two to four times the rate of people who are not adopted. The real question should be why does our society only care about certain favoured groups? Our society clearly isn't interested in lowering suicide rates, except among the favoured groups.